Latest technology for mapping abnormal heart rhythms
The technology we use in medicine is always evolving. Since I started working in the field of heart rhythm management, there have been incredible advances in the equipment and computer technology, which have revolutionised our ability to treat patients.
When dealing with complex heart rhythm disturbances, one of the treatment options is catheter ablation. We can use 3D mapping systems to superimpose anatomical and electrical information onto a 3-dimensional shell of the relevant part of the heart, usually the specific chamber where the rhythm is coming from.
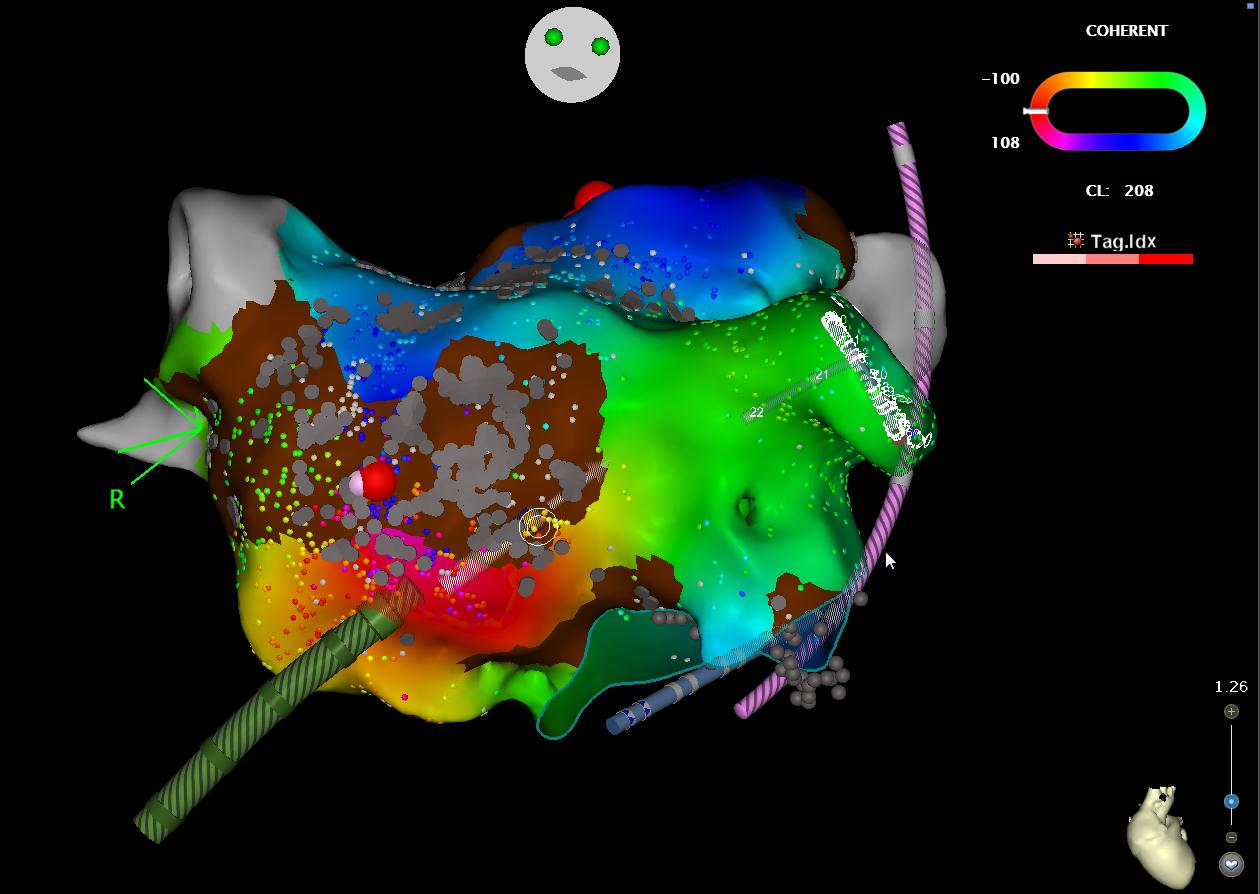
An example is shown here. Fine catheters are passed to the heart from the blood vessels at the top of the leg, using a keyhole technique. We can then reconstruct the shape of the chamber in question, and acquire multiple timing points within the chamber in order to work out how the rhythm disturbance (or “arrhythmia”) is happening. The timing points are colour-coded by the system to show the sequence in which the rhythm passes across the chamber (red – orange – yellow – green – blue).
In this example, the left atrium (upper collecting chamber) is shown. The area coloured brown represents an area of scarring. The circuit causing the arrhythmia is passing through this area of scar, and then passes around each area in a “figure of eight”. You can identify this if you follow the colours in order (red – orange – yellow – green – blue). A single localised burn between the areas of scar was enough to stop the faster rhythm and restore the normal rhythm, leading to the patient’s symptoms being resolved.